kaiser permanente appeal form
Complete the Member Appeal Request form PDF and return it to the Member Appeals department using one of the following delivery options. PROVIDER APPEALS RESOLUTION REQUEST.

Kaiser Provider Appeal Form California Fill Online Printable Fillable Blank Pdffiller
Medicare Advantage Appeals Process Level WrittenVerbal Resolution Maximum timeframe from contact date not including extensions.
. You may deliver the form in person or by mail. Original Claim Amount Paid. Appeal Decision Timelines.
Provider reconsideration process The claims payment review and reconsideration steps include. Kaiser Permanente Member Appeals PO. Depe Mental Health iti scrib Initials scrib.
Mid-Atlantic Claims Administration Kaiser Permanente. Once a decision has been made the providers appeal rights are exhausted unless additional documentation to support the appeal is supplied to Kaiser Permanente subsequent to the Appeal Units decision. If you need an expedited appeal due to a life-threatening situation call us.
How to Appeal Mail PO. Antioch CA 94509. 3Get a payment receipt for services which can be a receipt from your provider a copy of the check or a bank or credit.
Kaiser Foundation Health Plan Inc in Northern and Southern California and Hawaii Kaiser Foundation Health Plan of Colorado Kaiser Foundation Health Plan of Georgia Inc Nine Piedmont Center 3495 Piedmont Road NE Atlanta GA 30305 404-364-7000 Kaiser. Health Care andor Financial Dependent Power of Attorney form stipulating you are currently authorized to appeal on behalf of the member. Appropriate Appeal Submission Addresses.
Kaiser Permanente of Colorado Provider Appeals PO. If you are the treating provider submitting this request on behalf of a member you must submit an. 2Get an itemized bill from your provider detailing the charges see Section B for the information needed in this bill.
Kaiser Permanente Provider Appeals Provider Contracting and Relations 500 NE Multnomah Blvd Ste 100 Portland OR 97232 503-813-3376 503-813-2017 Fax. Appeal is submitted without Appeal Filing Form the information listed below must be present. Patient Date of Birth.
1 your name and your Medical Record Number. Kaiser Permanente Medical Record Number. Information on how to submit changes or updates to your provider information so Kaiser Permanente can maintain an accurate provider directory.
Please contact Member Appeals at 1-866-458-5479 if you need a copy of this form. Then you must send Kaiser Permanente Member Appeals. Please return form to.
Please return this form to your local Kaiser Permanente Member Services department for processing. 1Fill out this form completely and sign it. Signature Select Added -Choice Flexible Choice Option 1 Medicare Advantage and Medicare Plus.
You contact our health plan and make your appeal. 5855 Copley Drive Suite 250. Member Services Main Office.
AG1000097-01-17 Kaiser Foundation Health Plan of Washington. Please note that all claim payment appeal requests must be filed within 365 days of the date the claim was originally processed or denied in order to be considered for payment by Kaiser Permanente. Keep a copy for your records and submit the original toKaiser Permanente Appeals POBox 34593 Seattle WA 98124-1593.
Box 34593 Seattle WA 98124-1593. Select an area California - Northern California - Southern Colorado Colorado - Denver Boulder Northern Mountain areas Colorado - Southern Colorado Georgia Hawaii Maryland Virginia Washington DC. And 4 the specific reasons for your request that we review our initial decision.
Appeal Submission Address for Coverage Plans Listed Below. Kaiser Foundation Health Plan Inc in Northern and Southern California and Hawaii Kaiser Foundation Health Plan of Colorado Kaiser Foundation Health Plan of Georgia Inc Nine Piedmont Center 3495 Piedmont Road NE Atlanta GA 30305 404-364-7000. Street City Zip Code Daytime Telephone Number.
HMO- Center or Network-Based PCP. Address Medical Record Number. GrievanceAppeal FORM - Medicare Northern California MemberPatient Name.
Tell us where the issue happened. Seattle WA 98124-1593 ATTN. Call Member Appeals Toll-Free 1-866-458-5479.
Kaiser Permanente Health Plan Coverage Options. Kaiser Permanente Claim ID Number. As outlined in the Appeal Rights please include in your request.
Kaiser Permanente health plans around the country. Member Services Main Office. Reason for denial member name medical record number service dates and.
3 the specific treatment service or supply that you are requesting. Appeal and action taken by the Kaiser Permanente Appeals Unit. Name of Person Filing If.
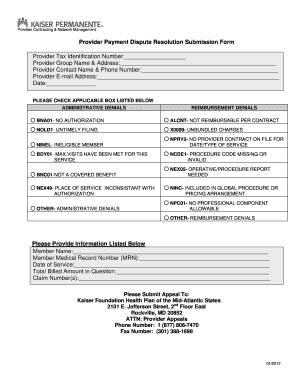
GrievanceAppeal FORM - Medicare Southern California MemberPatient Name. An inventory of all forms for health services billing and claims referrrals clinical review mental health provider information and more. Box 372970 Denver CO 80237 PROVIDER- CARRIER DISPUTEAPPEAL FORM Please complete the following information for each disputed claim Date.
Kaiser Permanente health plans around the country. Members who receive a denial reduction or limitation notice for services may initiate an appeal within the specified time period as described in their. Submit your request for a standard appeal in writing by fax mail or online through the Kaiser Permanente member website see below for contact information.
Form requests 1 800 810-4766 General claims status and payment inquiries Clarification of member benefits Provider appeal status Members presenting with no Kaiser Permanente identification card Members terminated for greater than 90 days. 3400 Delta Fair Blvd. Original Claim Amount Billed.
2 your medical condition or symptom. Oregon SW Washington Washington. HMO- Center-Based PCP.
Sign in to the secure Kaiser Permanente member website and submit the Online Member Appeal Request. Kaiser Permanente Signature. GrievanceAppeal FORM - MedicareSouthern California.
KP HAWAII PROVIDER APPEALS CLAIMS ADMIN DEPT PO BOX 378021 DENVER CO 80237-9998. San Diego CA 92111.
July 21 2012 Getty Owl Foundation
Kaiser Provider Appeal Form California Fill Online Printable Fillable Blank Pdffiller
2
Kaiser Permanente Combined Disclosure Form At Your Service
2
2

Get And Sign Can I File A Motion To Extend Perfect Appeal For State Of Virginia Form
2
Claims 8 0 Kaiser Permanente
2
2
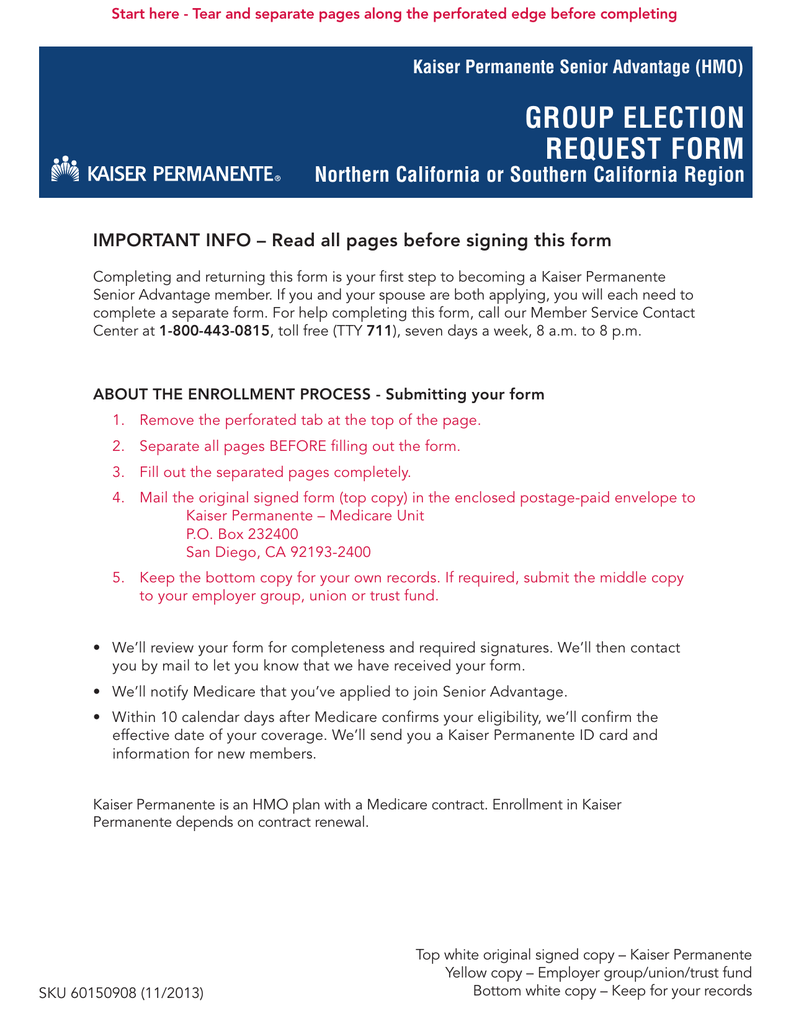
Group Election Request Form Northern California Or Southern California Region
2
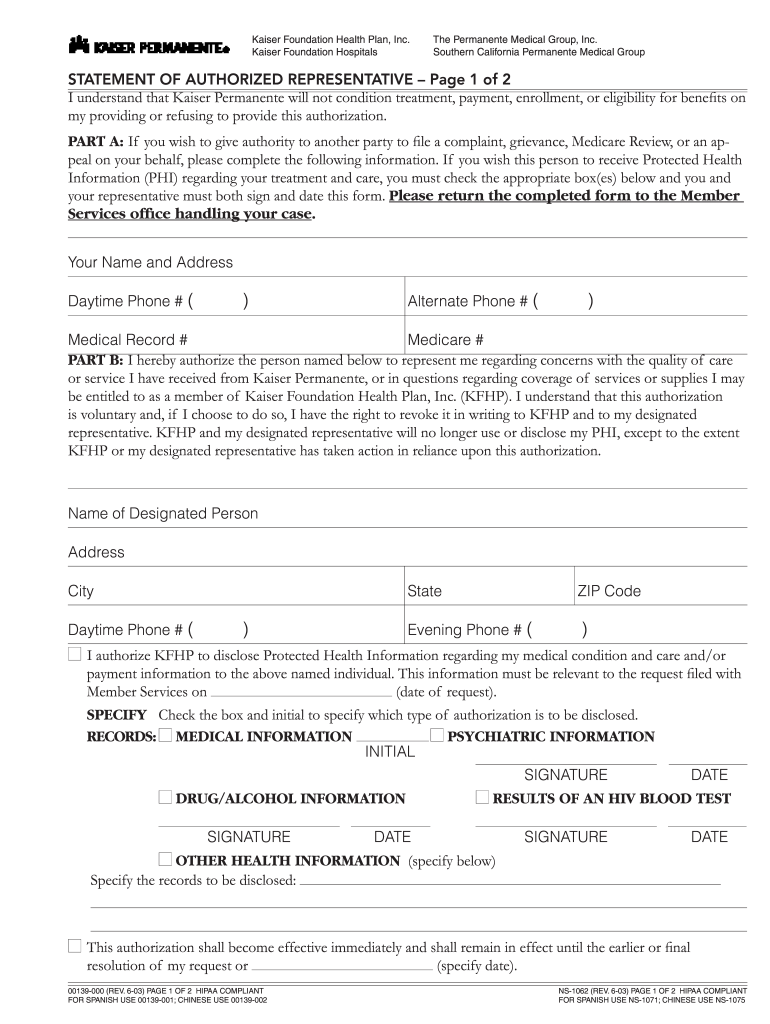
Kaiser Permanente Ns 1062 2003 2022 Fill And Sign Printable Template Online Us Legal Forms
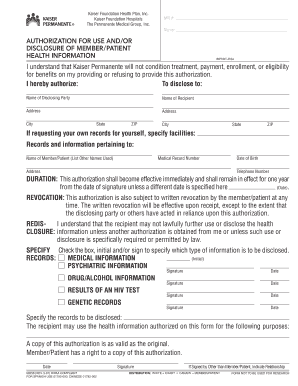
Fillable Online Mydoctor Kaiserpermanente Kaiser Permanente Authorization For Use Or Disclosure Form Fax Email Print Pdffiller
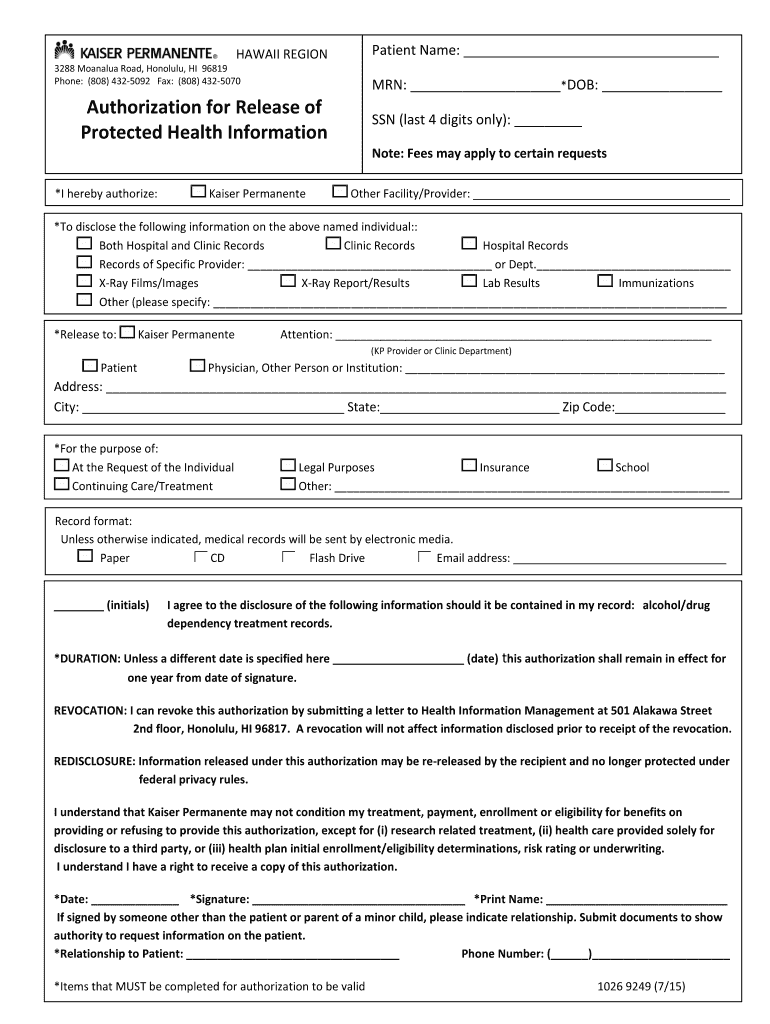
Kaiser Medical Records Fax Number Fill Online Printable Fillable Blank Pdffiller
Wa State Kaiser Fax Cover Sheet Form Fill Online Printable Fillable Blank Pdffiller
Kaiser Permanente Grievance Form Southern California 2020 2022 Fill And Sign Printable Template Online Us Legal Forms
Application Kaiser Permanente California